Torpor, Not Cryonics: A Real Path to Long-Duration Flight—and Earthside Payoffs
Unlike the imaginary use of cryonics in science fiction films and entertainment, induced deep sleep (torpor) is within the realm of our technological capability.
Credit: 20th Century Fox / Disney / Alien
Induced hibernation protocols plus organ “nanowarming” point to practical value now
Full cryo-preservation and restoration of astronauts makes for compelling sci-fi. The actionable programme for the next two decades is induced deep sleep states or torpor—lowered metabolism and core temperature for transit phases—paired with medical hardware and infection-control protocols you can certify. Through NASA’s NIAC-funded studies, SpaceWorks have quantified vehicle-level wins (figure 2): mass and consumables reductions, smaller habitats, and simplified life support, with detailed design trades for torpor habitats and even concepts that pair torpor with artificial gravity. ESA’s analyses reach similar conclusions: hibernation could cut spacecraft mass by a third and improve crew health by reducing activity-related stressors. This is engineering you can plan against, not cryonics speculation.
The medical base case isn’t exotic: hospitals already use targeted temperature management (TTM) after cardiac arrest. Guidance has evolved, but modern statements converge on strict fever prevention and controlled temperature management (32–37.5 °C) for at least 24 hours, embedded in full ICU care bundles. Torpor research extends these principles to weeks or months, which requires answers on sedation, nutrition, infection control, pressure injury prevention and safe re-warming—but the clinical scaffolding exists. For buyers—spacecraft integrators and mission insurers—that distinction matters.
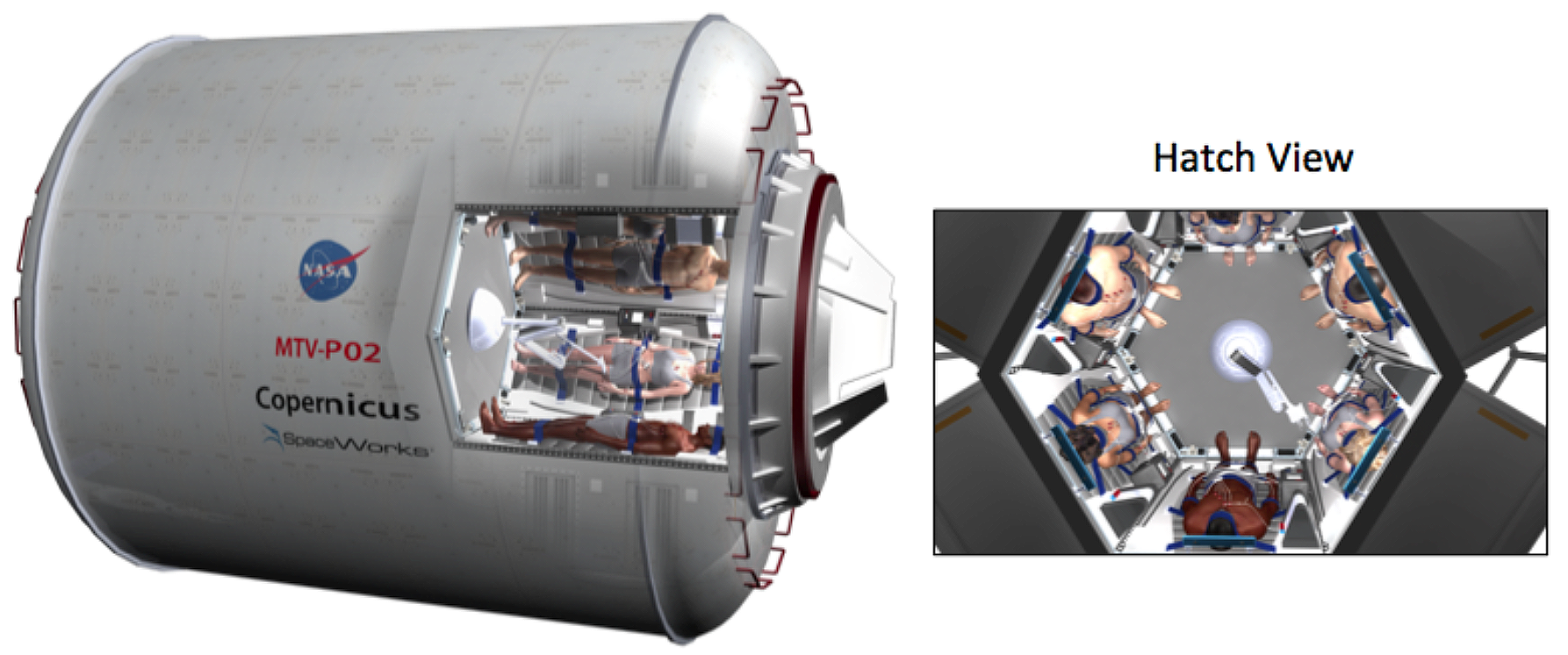
Figure 2: SpaceWorks’ torpor habitat design for transporting crews between the Earth and Mars is capable of cycling the crew through inactive, non-cryonic torpor sleep states for necessary durations of space travel.
Credit: J. Bradford / SpaceWorks Engineering, Inc.
Where does the “cryopreservation” narrative become real? In organs, not whole humans. In 2023, a University of Minnesota team demonstrated vitrification + nanowarming of rat kidneys with successful life-sustaining transplantation after up to 100 days of storage—the first repeated proof that a complex mammalian organ can be banked at cryogenic temperatures and returned to function. The commentary in transplant journals and news coverage called it a seminal milestone; challenges remain to scale to human organs, but the pathway is clearer than at any time in the field’s history.
Commercial implications break into two tracks. In space, torpor becomes a service contract: protocols, hardware (cooling, monitoring, RF-safe devices), consumables and training, integrated with ECLSS and the flight surgeon’s playbook. Vendors who show ICU-grade artefacts (alarm trees, dosing algorithms, re-warming curves, infection bundles) and a step-wise trial plan earn trust: ground analogues → parabolic/bed-rest studies → lunar-transfer durations. On Earth, the wins are immediate: torpor-adjacent tech can extend golden hours for austere/remote medicine and transform organ logistics if nanowarming scales, expanding transplant access and reducing discard rates. Hospitals and ambulance networks can justify spend on the same monitoring, temperature-control and anti-shivering stacks you’d need in space.
A buyer-friendly go-to-market reads like this. Start with temperature-control platforms and monitoring software that meet current AHA/ILCOR norms; add research-only torpor extensions with clear guardrails. Partner with transplant-science groups to productise nanowarming peripherals (nanoparticle prep, RF coils, perfusion protocols) and publish head-to-head metrics: storage days, graft function, adverse events. For mission planners, package torpor as risk-reduced life support with mass/volume savings, documented in NIAC/ESA studies. That combination—credible medicine + mission economics—is how torpor becomes part of real flight plans and a revenue line on Earth.
The bottom line: keep developing cryonics but skip the hype. Until then, induced torpor and organ nanowarming give near-future space programmes tangible advantages and give Earth medicine new tools worth funding now. Put your effort where regulators and clinicians will meet you: protocols, devices, and data that line up with today’s standards—and scale patiently from there.